severe osteo-arthritis
This is a case of severe mulitple joint Osteoarthritis which Mr. Ryals managed with conservative treatment modalities.
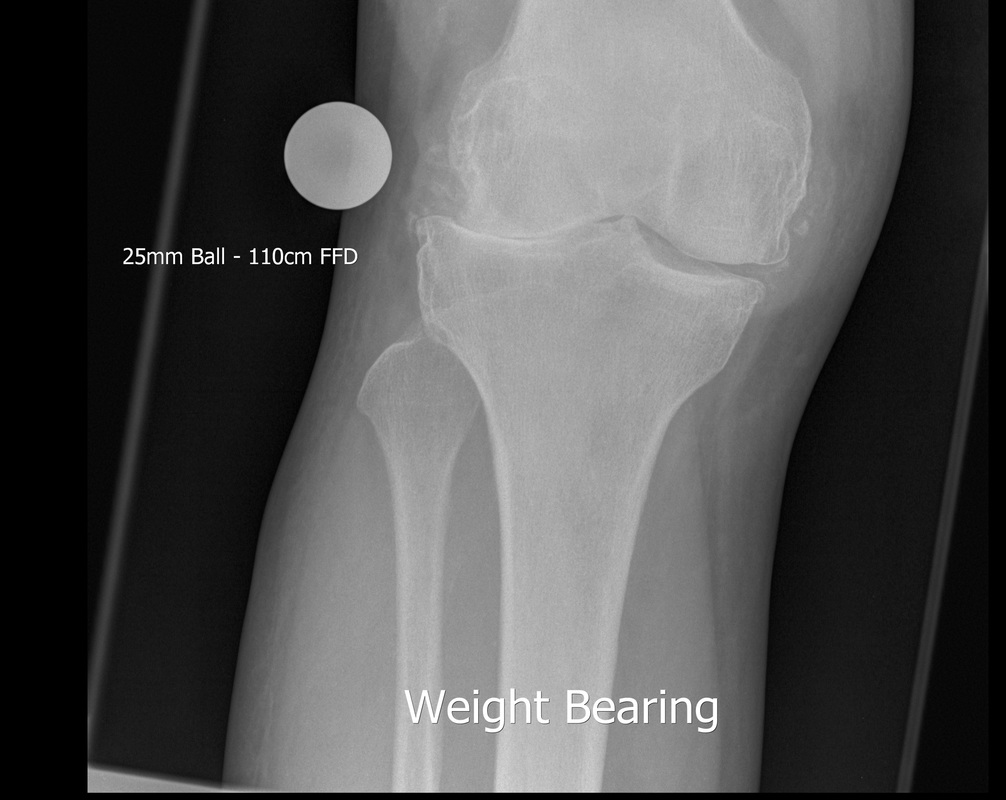

The first two X-Rays to the left shows complete degeneration of the lateral meniscus (cartilage) of the right knee. This X-ray was a standard weight bearing AP view of the knee to assess severity of the patients arthritis and to review treatment options. Previously an Orthopaedic surgeon had recommended complete knee replacement. The second Xray show a partially weight bearing "Skyline" view of the same patients right patellofemoral joint. This X-ray shows complete destruction of the medial articular facet of this particular joint alongside large painful osteophyte formation along the periphery of the patella.


The X-ray to the left shows a standard weight bearing AP view of the right Subtalar and ankle complex an unusual medial tilt to the talas can be seen alongside complete destruction of the articular cartilage between the tibia and talus. The second X-ray to the right shows a standard weight bearing lateral view of the Subtalar and Calcaneocuboid joint, again large swathes of Osteoarthritic damage can be seen to the joint. Clinically the Subtalar joint has a reasonably well preserved range of motion. Pain was rated as being severe in all the joints with the patient scoring 90%+ on a visual analouge scale. An orthopeadic surgeon had basically offered the patient a total knee replacement alongisde a clean out of the patella and a triple ankle joint athrodesis to remedy the patients pain and arthritis. The patient sought a second opinion from Mr. Ryals with regards alternate forms of treatment.
MANAGEMENT
Knee AND PATELLA

Mr. Ryals organised for a GP colleague to perform a simple athrocentesis procedure to drain the patients swollen painful right knee, this was also to be injected with simple Coritcosteroid injection. These injection were organised to reduce pain and inflammation whilst trying to restore some function to the joint. The same procedure was performed to the right patellofemoral joint. The patient had not been offered Synovial fluid replacement therapies. It was decided to assess the effects of the athrocentesis and steroid injection before additional joint injections.
ANKLE
It was decided that a similar management plan would be organised for the right subtalar joint but with the additional administration of simple ostenil injections. Once again a simple athrocentesis was performed to the right Subtalar joint alongside adminstration of a steroid injection. It was decided to leave further Ostenil injections into the right Subtalar joint for several weeks to assess the effects of the athrocentesis and steroid injection.
OUTCOME
A review appointment was made for four weeks on the proviso the patient was to contact the clinic as soon as possible if they became symptomatic. Close questioning of the patient revealed a marked improvement to the right knee and they reported a VAS score of 4 which was orginally above a 9, so an approximate 50% improvement. The right subtalar joint didn't quite fair as well and scored a 6 on the VAS, so again an approximate 30% improvement. The patient requested Ostenil injections into the right Subtalar joint. The patient recieved three injections of 1mg Ostenil mini over the next three weeks. Another appointment was organised to review both the knee and ankle in another four weeks. The second review revealed no further improvements to the right knee but the patient was happy with the outcome and reported that they used anti-inflammatory medications for "bad days". The right ankle joint improved slightly from the previously reported score 6 on the VAS down to a 5. The patient was happy with the overall outcome of the injections and was considering additional orthotic management.
It was decided that a similar management plan would be organised for the right subtalar joint but with the additional administration of simple ostenil injections. Once again a simple athrocentesis was performed to the right Subtalar joint alongside adminstration of a steroid injection. It was decided to leave further Ostenil injections into the right Subtalar joint for several weeks to assess the effects of the athrocentesis and steroid injection.
OUTCOME
A review appointment was made for four weeks on the proviso the patient was to contact the clinic as soon as possible if they became symptomatic. Close questioning of the patient revealed a marked improvement to the right knee and they reported a VAS score of 4 which was orginally above a 9, so an approximate 50% improvement. The right subtalar joint didn't quite fair as well and scored a 6 on the VAS, so again an approximate 30% improvement. The patient requested Ostenil injections into the right Subtalar joint. The patient recieved three injections of 1mg Ostenil mini over the next three weeks. Another appointment was organised to review both the knee and ankle in another four weeks. The second review revealed no further improvements to the right knee but the patient was happy with the outcome and reported that they used anti-inflammatory medications for "bad days". The right ankle joint improved slightly from the previously reported score 6 on the VAS down to a 5. The patient was happy with the overall outcome of the injections and was considering additional orthotic management.